




Risks and limits of surgery
Do I need a breast lift or a breast reduction?
When I see you in clinic I will assess you carefully to check both the size of your breasts and the amount of drop that has occurred. If in a well-fitted supporting bra you are happy with the size of your breasts then you do not need a breast reduction rather a breast lift alone will suffice. If you feel that your breasts are too large then a breast reduction is the correct procedure for you particularly if accompanied by other symptoms.
How do I choose what size to go down to?
Breast reduction is a procedure that requires experience as the aim is not just to reduce the size of the breasts but to also maintain a pleasing breast shape. This requires skill, experience and technical ability. When I assess you I will take into account a number of factors which will affect the size of your breasts. Most important of these is the size that you yourself wish to aim for. This may require some modification according to your build and the width of your chest. For example if you have a very wide base to your breasts (a common finding when the breasts are large) reducing the breasts too much will lead to a very flat shape to the chest and although you may experience relief from the symptoms of heavy breasts the benefits will be short lived because of the loss of breast shape that will follow. In this situation it is advisable to limit the breast reduction to that which still maintains an aesthetic breast shape. There are further modifications which can be used to improve breast shape that are technical. For example my own technique involves removing more tissue from the outer lower aspect of the breasts (towards the armpit) and maintaining as much as possible on the inner aspect of the breast so that whilst the breasts are reduced in size a degree of cleavage can be maintained?
I am worried about the scars from a breast reduction
Over the many years that I have been carrying out breast reduction my experience is that women are more than happy to accept the scars given the great benefits that the operation offers. As far as possible I use techniques to minimise the impact of the scars. The horizontal scar in the breast fold is generally tucked away out of vision. I take time using a fine buried suture technique to close the wound around the areola and the vertical scar to minimise the impact of this scar. After surgery it is important that you follow my instructions for managing your scars. Essentially you should massage your scars once healed twice a day with a moisturiser and firm pressure to reduce the chance of thickening of the scars. If you are in a sunny environment it is important that you put a layer of sun block over your scars to prevent them from becoming reddened or pigmented. These measures should be carried out for a period of 12 months and in most patients scarring from this operation is very acceptable.
What happens if I become pregnant?
Pregnancy may enlarge your breasts again and tend to undo the effects of the operation. It is sensible therefore to time your surgery with this in mind.
I am losing weight. Will this affect my breast reduction?
It is important with most cosmetic procedures that your weight is stable before you embark on them. Many women who are losing weight will find that they lose a good deal of that weight from their breasts. In contrast other women find that weight loss does not affect their breasts at all. My advice to women in the first category is that you should complete any weight loss programme prior to embarking on breast reduction. This has advantages in that excess skin can be removed and the breasts lifted to an optimum degree once you have completed your weight loss and secondly less tissue will need to be removed if you have lost weight already from the breasts. Both of these would result in a better result. If you are in the second category in which weight lose does not affect your breast then the timing of the operation is less critical. I would advise however again that if possible you do lose whatever weight you are planning to lose.
Will I be able to breastfeed after breast reduction?
The technique that I use in the vast majority of women is the inferior pedicle technique in which a mound of breast tissue with the nipple and areola attached is preserved, thus the breast ducts and nerves to the nipple and areola are also preserved. This means that this operation has in my view the least effects on the remaining breasts and if you were able to breastfeed before, the chances are you will be able to breastfeed after this operation. Similarly if you had good nipple sensation before it is likely you will have a good nipple sensation after. It is important to note however that in some patients the breasts can become hyperesensitive presumably because the breasts have been lifted and there is less weight on the nerves.
Are there any complications from this type of surgery?
Breast reduction like all operations carries a risk of complications and I will go through these with you in detail at your consultation.
Aftercare
Women with heavy breasts may experience a number of symptoms which include discomfort in the neck, shoulders and back from supporting extra weight. Bra straps that cut into the shoulders, sweating, rashes and skin infections in the fold underneath the breasts and generalised breast pain. In addition women report difficulties in buying clothes and underwear that fit due to the disproportionate size of the breasts.
Heavy breasts may rest on the abdomen giving a false impression of abdominal obesity and emptiness in the chest region. Apart from these physical symptoms there are significant psychosocial factors associated with large breasts.
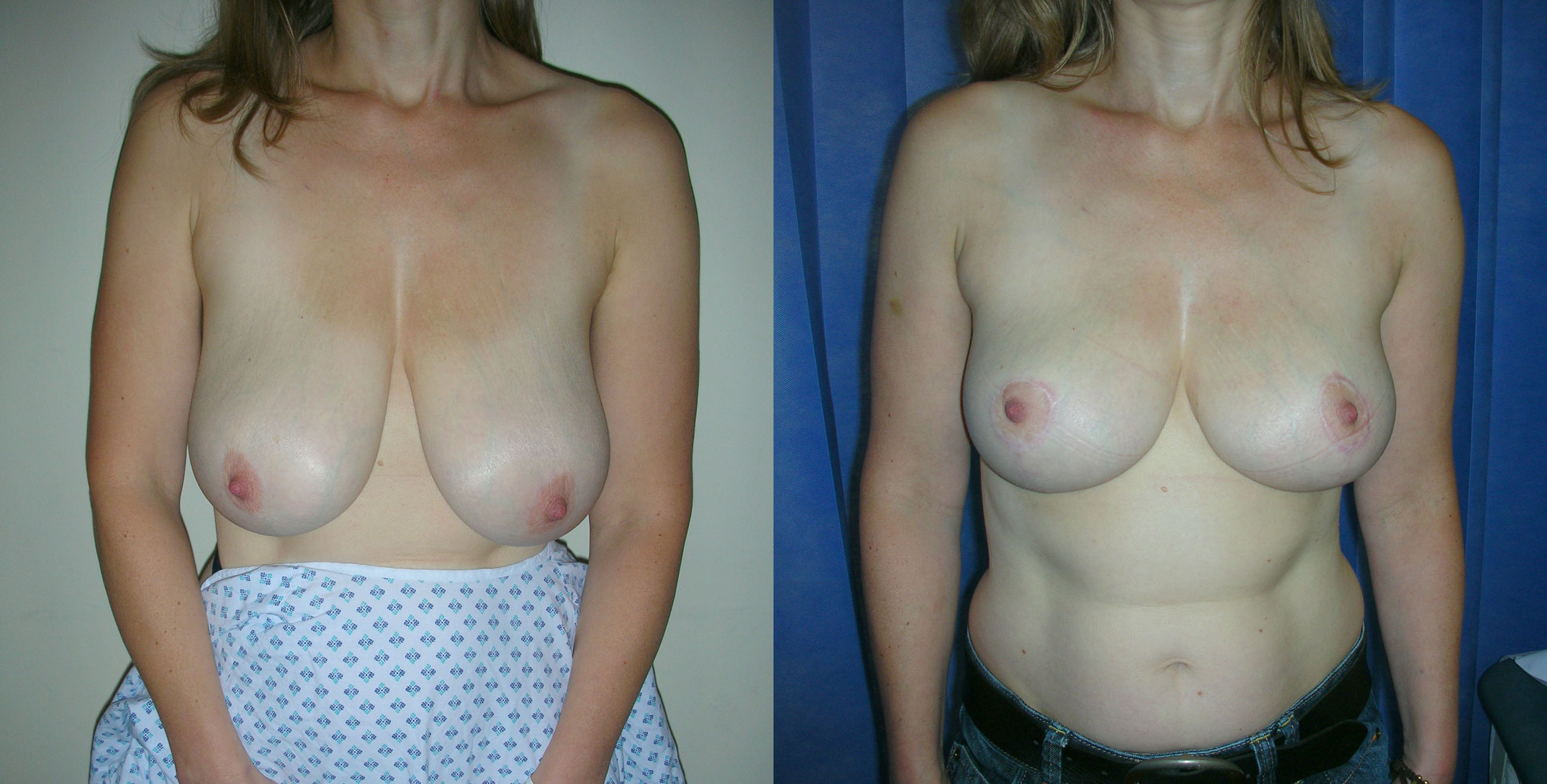
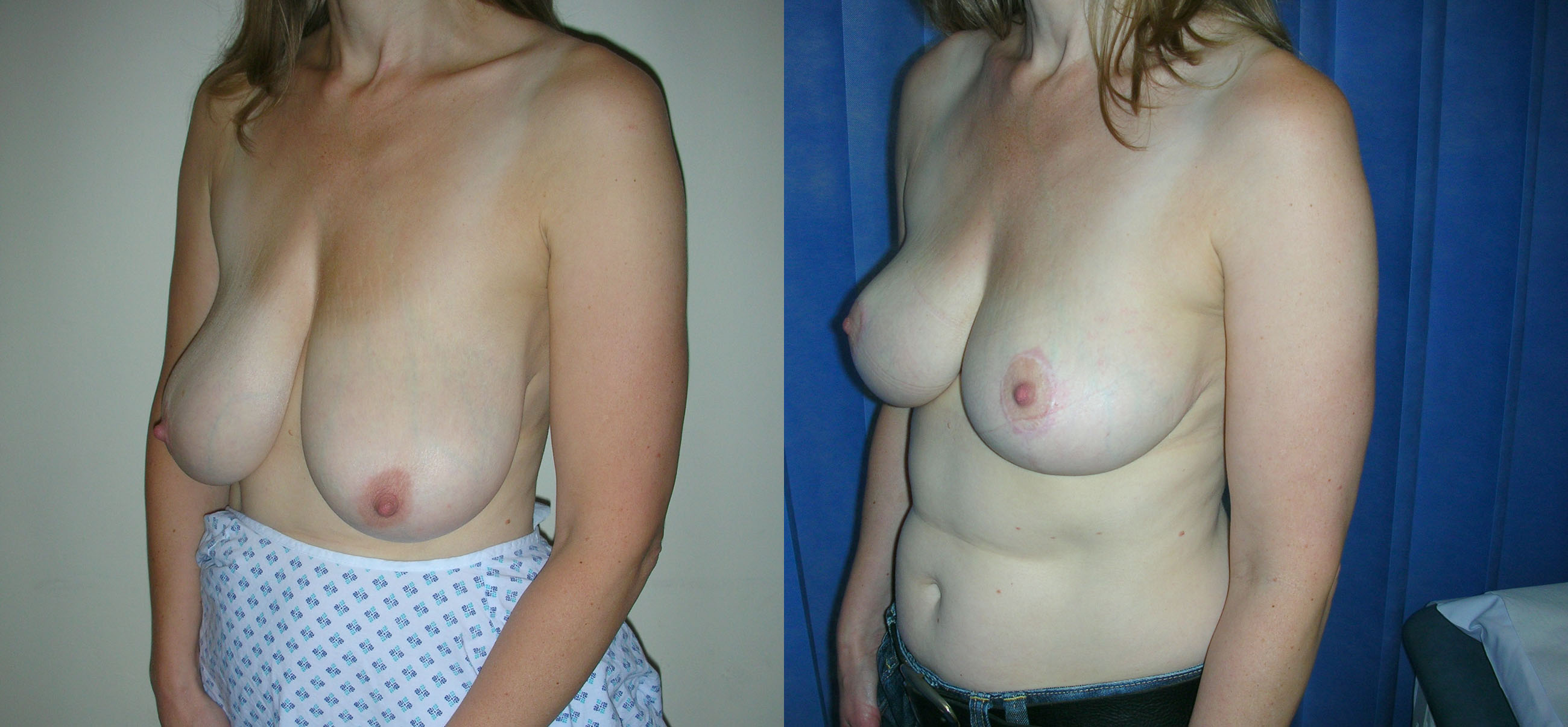
Breast reduction makes two changes to the breasts. Firstly it reduces the size of the breasts and secondly it lifts the breasts. The degree of reduction and/or lift is tailored to your individual circumstances. All of these can be improved by breast reduction. If you seek to reduce the size of your breasts then a breast reduction is the correct operation for you. If your breasts have sagged due to stretching of the skin over time, weight loss, the effects of pregnancy, then a breast uplift may be more appropriate. In this situation the breasts are lifted without reducing the size.
There are many different techniques of breast reduction. In practice however there are only two major differences between the various operations. The commonest approach is that in which the nipple and areola are preserved on an internal mound of breast tissue and this is repositioned having been reduced in size with shaping of the surrounding breast tissue and skin. This approach has the advantage that it is often possible to preserve the nerve supply (and thus the sensation) as well as the breast ducts (therefore the ability to breastfeed) to the nipple areola. The second approach is used far less commonly is generally reserved for patients whose breasts are extremely large or extremely drooping. In this approach the nipple-areolar complex is removed as a graft, the breast reshaped and the nipple areola grafted back into the correct position on the newly shaped breast.
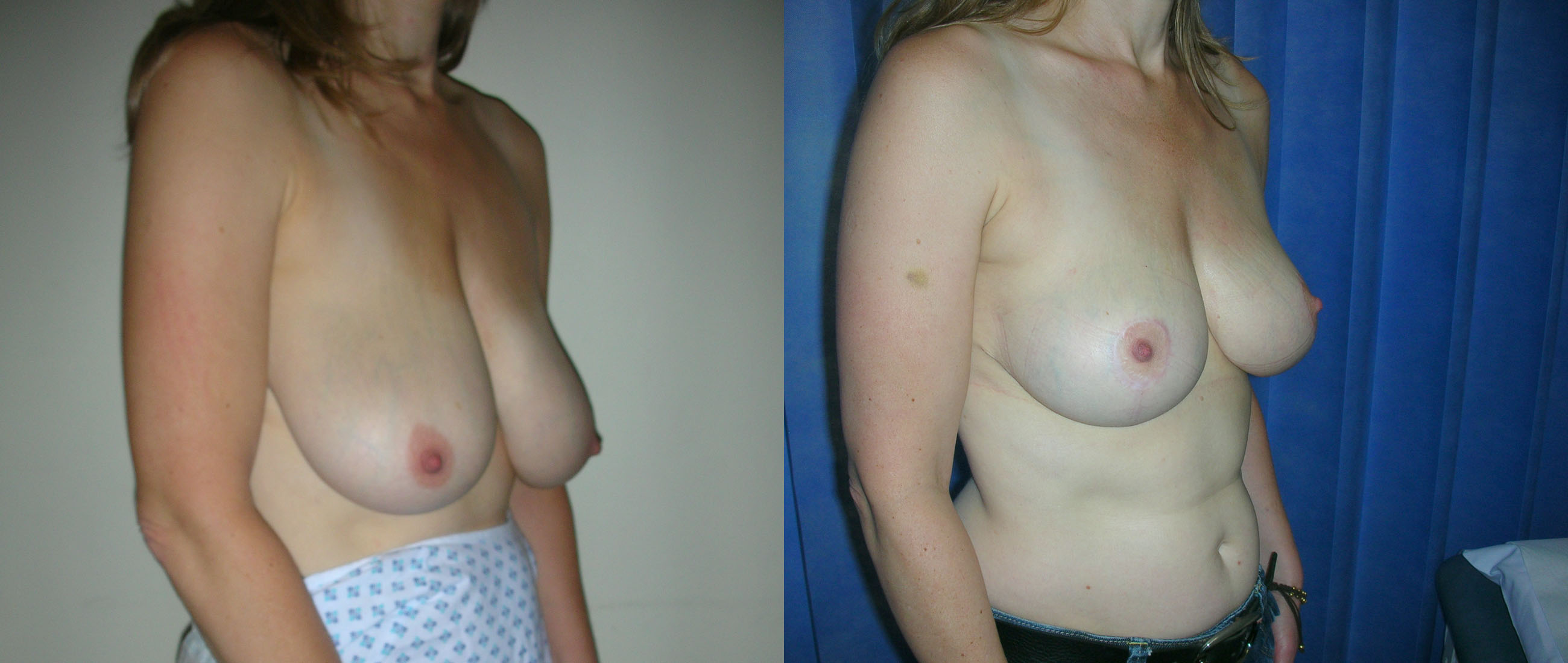
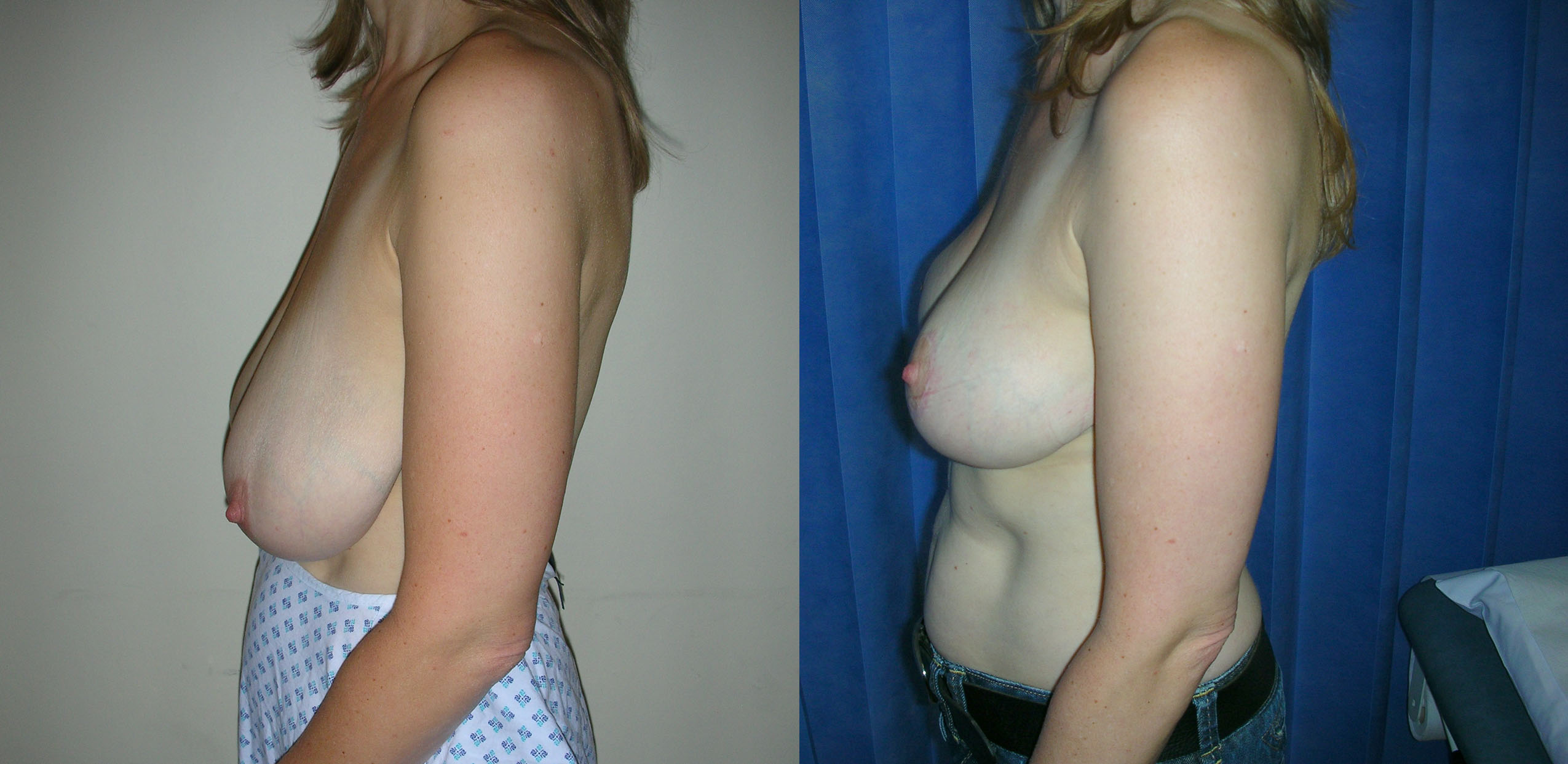
Breast reduction is carried out under general anaesthetic and takes two to three hours to carry out. When the breasts are larger the procedure may take longer. At the end of the procedure I put a small silicone tube (surgical drain) into each breast and I usually leave this in place for 48 hours. The hospital stay is for two nights. The scars from a breast reduction vary according to the technique used. In the technique that I use most frequently the scar circles the areolar edge, passes vertically down to the breast fold and runs along the whole length of the fold.
Breast reduction can also be used to correct or improve major asymmetries of the breast. Whilst minor asymmetries are very common (most women will have one breast a little larger than the other or of a different shape than the other). When this is significant breast reduction can improve the appearance.
When I see you in my clinic I will make an operative plan for you based on your general build, the size of your breast and the amount of droopiness to your breast taking into account your aims and personal preferences. Once we have established this plan I will go through all aspects of the procedure with you including recovery time for healing return to work, childcare and exercise. I will also go through potential complications and risks specific to you if you have any medical conditions. In preparation for your surgery it is helpful to have loose pyjamas or a large T-shirt to wear for your post-op stay. On the day of your operation I will meet you with my anaesthetist and we will go over your operation again and I will mark out your breasts in preparation for your surgery.
Once your operation is complete you will be taken to the Recovery Room where most patients wake up gently and are generally comfortable. As breast reduction does not involve entering any body cavities the discomfort following surgery is moderate rather than severe. Nevertheless you will be supplied with strong painkillers as required. Once you are fully awake you will be encouraged to get up and gently walk around. On your second post-operative day I will remove your drains and preparations will be made for your discharge from hospital. Your breasts will have dressings in place but at this stage I do not usually ask my patients to wear a bra. A loose T-shirt or top is ideal for the first week.
I ask my patients to keep their wounds dry and the dressings undisturbed for the first week. After this I will see you in my clinic and remove all the dressings and inspect your wounds. From this time onwards you can start to shower and apply a small amount of Sudocrem cream to your wounds. This acts as a barrier.
Following your breast reduction small areas of surface breakdown are not uncommon and Sudocrem is very effective at healing these quickly. They do not usually affect the long-term result.
At this stage you can start to wear a bra and I recommend that you acquire a supporting bra that is soft with no wires. This should be comfortable around the chest and slightly larger than your anticipated breast size to accommodate the swelling. During your first week at home it is important that you take plenty of rest but keep mobile. The simplest way to achieve this is walking both indoors and outdoors. You should avoid any heavy lifting and any vigorous activities including the gym. It is important to note that this operation has a significant impact on your ability to carry out shopping, household duties and childcare particularly in the first two weeks. After a week to 10 days you may drive for short essential trips and following two weeks you can usually build up to your normal pattern of driving. If your work is office based or requires light duties only you may find you are able to return to work at two weeks. If your work involves any degree of heavy manual work I recommend that you take at least four weeks off.
During your recovery time I will keep a check on your progress in my clinic initially at one week then again at two weeks after your operation. This is followed by a four-week appointment and then one at three months to check how things are settling down. Following your breast reduction you should notice improvement in your posture if this has been adversely affected by the weight of your breasts prior to surgery, a more balanced shape to your body, an improvement in back, neck and shoulder ache and easier fitting for clothes. You may also find that exercise and sporting activities are more easily carried out.